









































Topical anaesthesia in ophthalmology
See p. 80.
Local infiltration
Many operations can be performed under direct infiltration of local anaesthetic at the operative site. Dilute solutions are quite effective and although large volumes may be required, toxicity is not a high risk, especially if epi-nephrine is added.
The simplest way is to inject the local anaesthetic step by step as the operation proceeds. Thus as the structures are exposed, they can be infiltrated under direct vision. For superficial operations such as herniorrhaphy, the whole procedure can usually be carried out after the initial infiltration, but if the patient complains of discomfort during the operation, more anaesthetic can be injected into the sensitive area.
Local infiltration for inguinal and femoral hernia repair
The repair of a hernia is easily accomplished by local' infiltration combined with blockade, of the ilioinguinal and iliohypogastric nerves. For the surgery to be painless it is necessary for the skin and muscle layers to be infiltrated together with anaesthesia of the hernial sac (which is parietal peritoneum) and, in males, the spermatic cord.
Anatomy
(Fig. 45:1).
Precautions
If possible the hernia should be reduced before starting the anaesthesia to avoid needle puncture of any gut lying within the hernial sac. If the hernia is strangulated, it may prove necessary to resect gut. This can be done with local infiltration, but will need further infiltration of the mesentery of the bowel under direct vision. Provided the patient is not dehydrated as a result of the strangulation, it may be better to consider a spinal anaesthetic.
If the hernia is very large, it may also be much easier to repair with spinal anaesthesia.
Technique for inguinal hernia repair
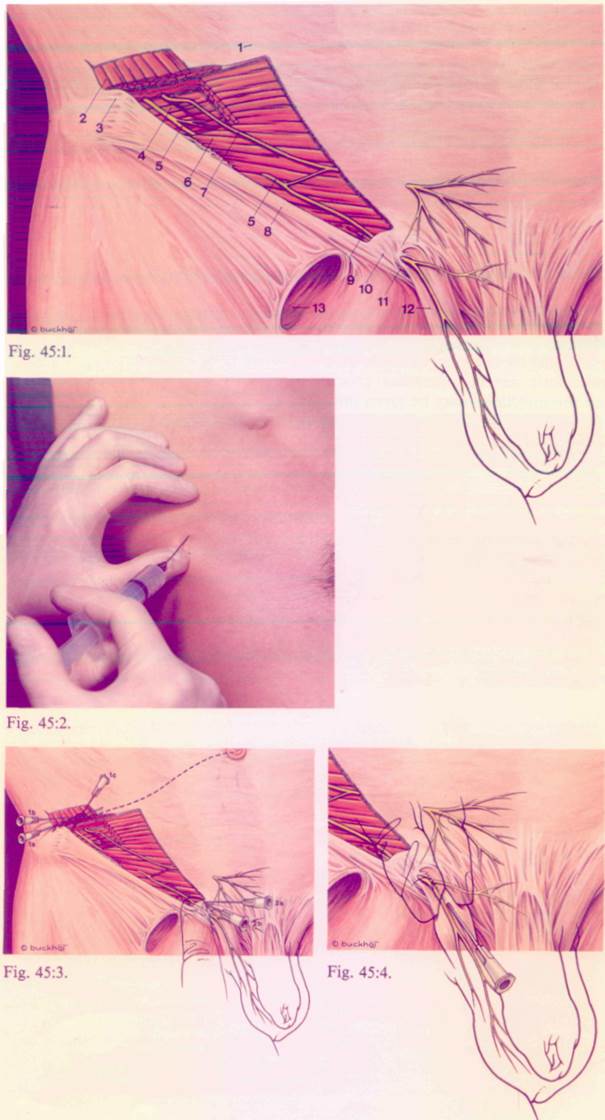
la. Raise a skin wheal 2 cm medial to the anterior superior iliac spine. Through this insert a needle towards the umbilicus and infiltrate (5 ml) subcutaneously (Figs. 45:2 and 3).
Ib. Repeat this injection (5 ml) deep to the external oblique anastomosis.
Ic. Direct the needle in the opposite direction so that it contacts the pelvic bone 1 cm deep to the anterior superior iliac spine. Inject 5 ml of solution, withdrawing the needle slowly. This injection should be made into the muscle tissue of the external and internal oblique muscles and the transversus. It will block the ilioinguinal and iliohypogastric nerves.
2a. Palpate the internal inguinal ring and inject 5 ml of solution into it (Fig. 45:3).
2b. Infiltrate 5-10 ml subcutaneously along the line of the incision (Fig. 45:3).
3. In males, pick up the spermatic cord at the external inguinal ring and inject 5 ml of solution directly into it. Apart from the normal contents of the spermatic cord, it will also contain the hernial sac. In females inject 5 ml above and medial to the pubic tubercle. (Fig. 45:4).
4. Further infiltration may be made under direct vision during the operation.
Technique for femoral hernia repair
Use the same technique as for inguinal hernia repair, omitting step 3.
Drugs and dose
Lidocaine 0.5%, prilocaine 0.5%, mepiva-caine 0.5%, bupivacaine 0.125%. Epinephrine 1:200.000 may be added. Total dose not to exceed 60 ml in an adult.
Fig. 45:1.
1. External oblique muscle
2. Internal oblique muscle
3. Anterior superior iliac spine
4. Transversus abdominis muscle
5. Iliohypogastric nerve
6. Inguinal ligament
7. Ilioinguinal nerve
8. Genital branch of the genitofemoral nerve
9. Spermatic cord
10. Pubic tubercle
11. Superficial inguinal ring
12. Inguinal hernia
13. Saphenous opening
Local infiltration for Caesarean section
While epidural or spinal blockade are widely used for Caesarean section, as is general anaesthesia, circunistances sometimes arise in which it is hazardous to use any of these methods. e.g. in cases of failed intubation, spinal deformity, massive bleeding or neuromuscular disease. It is worth bearing in mind that the operation can be performed using local infiltration with the mother conscious.
Anatomy
Fig. 47:1.
Method
The best results are obtained by infiltrating local anaesthetic as the operation proceeds. Thus all the injections may be given into the appropriate locations under direct vision. A little time (30-60 s) should be allowed for each injection to become effective.
1. Infiltrate the skin and subcutaneous tissue in the line of the incision (15.-20 ml). Incise the skin and expose the rectus sheath (47:2).
2. Infiltrate deep to the rectus sheath on the side of the proposed incision through the sheath (10-15 ml) (Figs. 47:3 and 4). The terminal branches of the intercostal nerves pass through the recti muscles and will be blocked, enhancing anaesthesia of the skin.
Fig. 47:1.
1. Anterior layer of rectus sheath
2. Rectus abdominis muscle
3. Posterior layer of rectus sheath
4. Linea alba
5. Median umbilical ligament
6. Parietalperitonium
7. Foetus
8. Anterior cutaneous branch
of the intercostal nerve
9. Uterine wall
10. Ttansversalis fascia
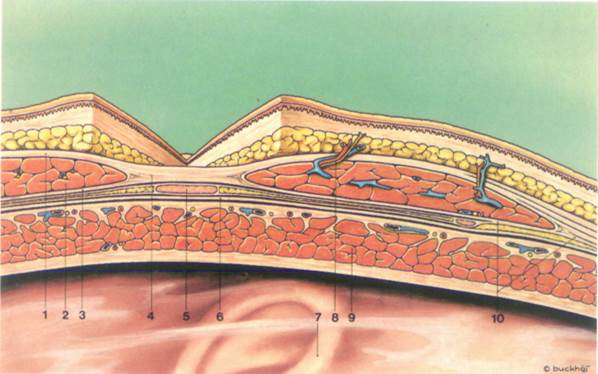
Fig. 47:1
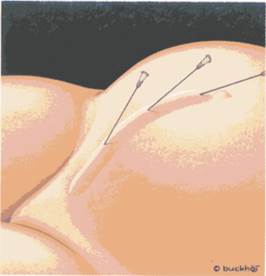
Fig. 47:2.
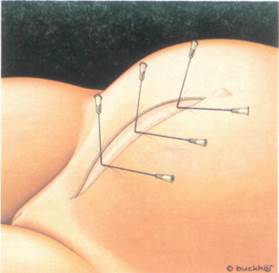
Fig. 47:3
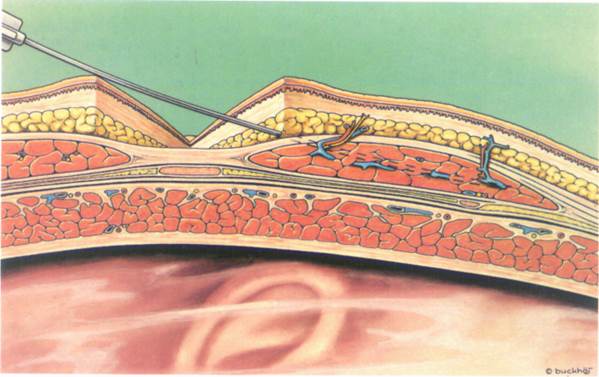
Fig. 47:4.
47
Уважаемый посетитель!
Чтобы распечатать файл, скачайте его (в формате Word).
Ссылка на скачивание - внизу страницы.