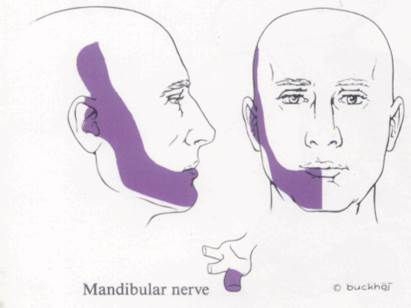
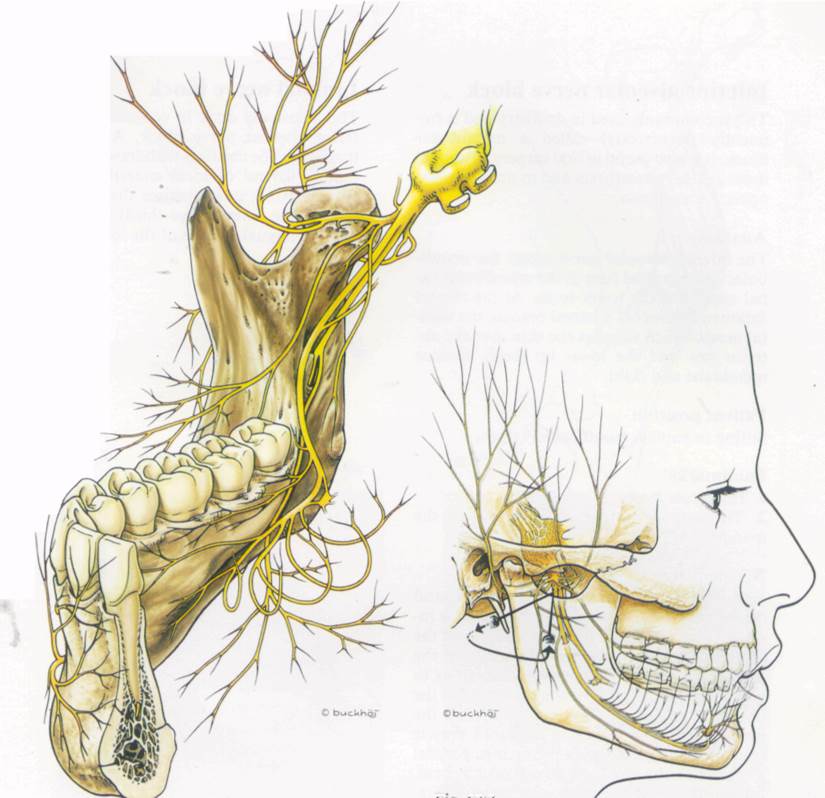
The posterior trunk divides into three branches, the auriculotemporal, the lingual and the inferior alveolar nerves. The auricnlotemporal nerve supplies the skin over the temporal region, the skin anterior to the ear (including the tragus) and the external auditory meatus (including the tympanic membrane). The lingual nerve supplies the mucous membrane of the floor of the mouth and the anterior two-thirds of the tongue, in addition to the lingual surface of the lower gums. The inferior alveolar nerve enters the mandibular foramen and runs in the mandibular canal supplying the lower teeth. At the mental foramen it gives off a lateral branch, the mental nerve, which supplies the skin over the anterior jaw and the lower lip (both mucous membrane and skin).
Patient position
Supine with head in neutral position, mouth closed.
Landmarks
1. The zygomatic arch
2. The condyle of the mandible
3. The coronoid process of the mandible
2 and 3 are identified by opening and closing the mouth.
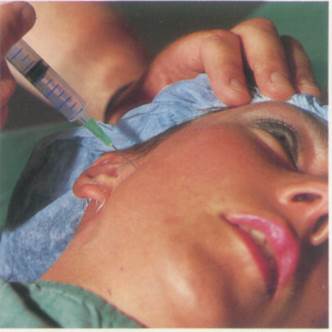
Needle insertion
A wheal is raised 0.5 cm below the zygomatic arch midway between the coronoid process and the condyle of the mandible. The needle is inserted at right angles to the skin until it contacts the pterygoid plate at a depth of 3-4 cm (Figs. 67:3 and 67:4). It is withdrawn a few millimetres and redirected 20° posteriorly until a paraesthesia is elicited.
Drugs and dose
5 ml of 2% lidocaine or 0.5% bupivacaine or their equivalent (see p. 20).
Fig. 67:1.
Fig. 67:2.
Fig. 67:3 Fie. 67:4
Inferior alveolar nerve block
This is commonly used in dentistry and is frequently (incorrectly) called a mandibular block. It is also useful in oral surgery to supplement genera,! anaesthesia and to provide postoperative analgesia.
Anatomy
The inferior alveolar nerve enters the mandibular foramen and runs in the mandibular canal supplying the lower teeth. At the mental foramen it gives off a lateral branch, the mental nerve, which supplies the skin over the anterior jaw and the lower lip (both mucous membrane and skin).
Patient position
Sitting or supine, mouth widely open.
Landmarks
1. The molar teeth
2. The anterior border of the ramus of the mandible
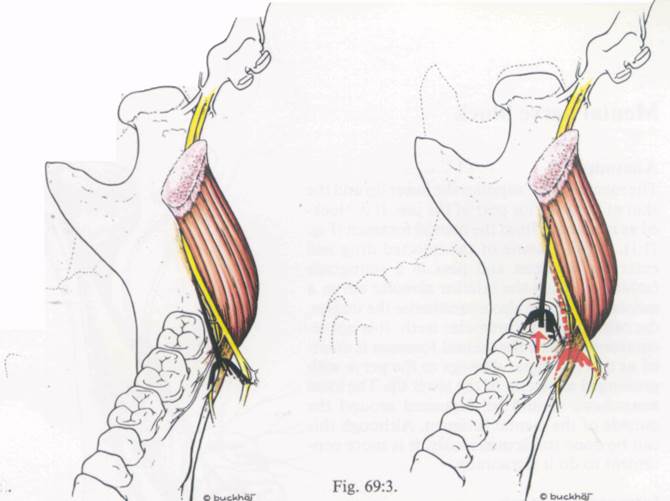
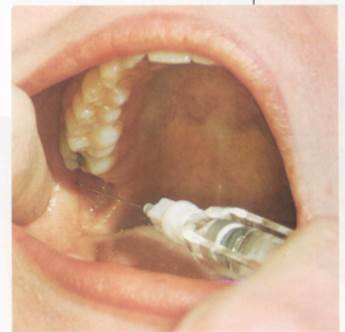
Needle insertion
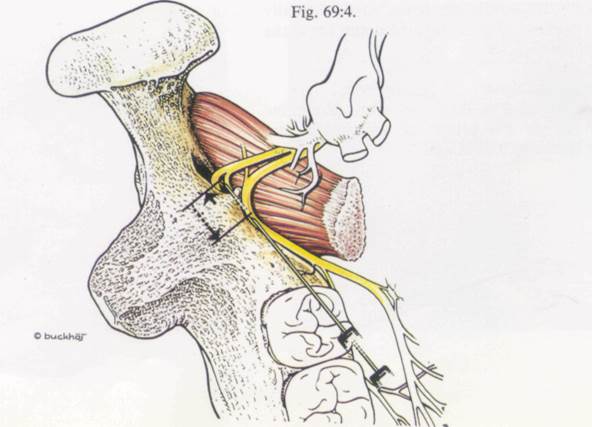
With the forefinger of the non-dominant hand on the ramus of the mandible the needle is inserted 1 cm above the occlusal surfaces of the molar teeth. The syringe is directed from the premolar teeth of the opposite side, so as to contact the medial side of the ramus. After the initial insertion, the patient should close the mouth a little to relax the pterygoid muscle (Fig. 69:1 and 3). Keeping the syringe parallel to the teeth the needle is advanced 1.5-2 cm, keeping the point in contact with the bone (Fig. 69:2). At the midsection of the ramus, resistance will be met. The needle is withdrawn 1-2 mm and the injection made (Fig. 69:4).
Drugs and dose
1.5-2 ml of 2% lidocaine with adrenaline 1:80.000 or 3% prilocaine with felypressin (Octapressin) 0.03 lU/ml. This is usually administered with a dental cartridge syringe.
Lingual nerve block
This is usually done in conjunction with inferior alveolar nerve block. After blocking that nerve, the needle is withdrawn 5 mm and a further 0.5 ml of local anaesthetic injected (Fig. 69:5). It anaesthetises the floor of the mouth, the anterior two-thirds of the tongue and the lingual surface of the lower gums.
Fig. 69:1
Fig. 69:2.
Fig. 69:5.

Mental nerve block
Anatomy
The mental nerve supplies the lower lip and the skin of the anterior part of the jaw. It is blocked as it emerges from the mental foramen (Fig. 71:1). Because some of the injected drug will enter the foramen and pass in a retrograde fashion to reach the inferior alveolar nerve, a mental block'will also anaesthetise the incisor, the canine and the premolar teeth. It is not recommended that the mental foramen is entered as this can cause damage to the nerve with prolonged analgesia of the lower lip. The local anaesthetic should be deposited around the outside of the mental foramen. Although this can be done transcutaneously, it is more convenient to do it intraorally.
Intraoral approach
Patient position
Mouth open and lower lip retracted.
Landmarks
Уважаемый посетитель!
Чтобы распечатать файл, скачайте его (в формате Word).
Ссылка на скачивание - внизу страницы.