22. Abdominal aortic plexus
23. Inferior mesenteric ganglion, artery and plexus
24. Superior hypo gastric plexus
25. Inferior hypogastric plexus
26. Pelvic plexus
27. Pelvic splanchnic nerve (nervus erigens)
28. Pudendal nerve
Figs. 213:3. Courtesy of Dr. D.G. Littlewood
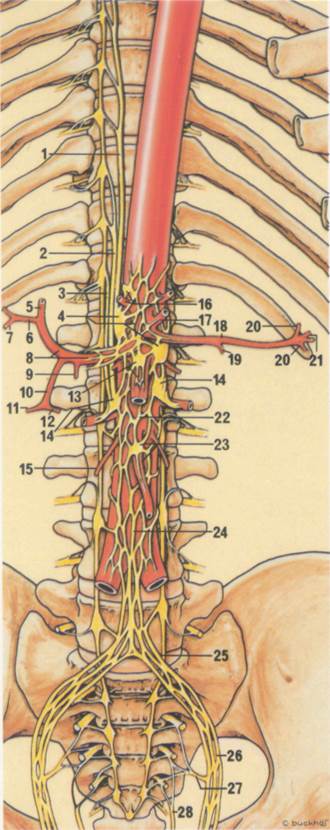
Fig. 213:1.

Fig. 213:2
Fig. 213:3.
Fig. 213:4.
Suggested further reading
Boas, R.A. (1978). Sympathetic blocks in clinical practice. In Regional Anesthesia: Advances and selected topics, Vol. 16, International Anes^Jiesia Clinics. Ed. Stanton-Hicks M. d'A. Little, Brown, Boston, p. 149.
Katz, J. and Renck, H. (1987). Handbook of Thoraco-abdom-inal Nerve Block. Mediglobe, Fribourg.
LOfstrom, J.B. and Cousins, M.C. (1988). Sympathetic neural blockade of upper and lower extremity. In Neural Blockade, eds Cousins, M.Cjjnd Bridenbaugh, P.O. Lippincott, Philadelphia, p. 461.
Moore, D.C. (1975). Regional Block. C. C. Thomas Springfield, Illinois.
I
£
Postoperative pain relief
One of the main advantages of regional anaesthesia is that following surgery the residual nerve block gives excellent postoperative pain relief as long as* the local anaesthetic drug maintains its effect. The duration of this residual block will of course be very variable, depending on the length of operation, the drug used and its dosage, the nerve block employed, etc. However, there are many ways in which the block may be extended to the patient's advantage.
The techniques do not have to be complicated, e.g. a ring block of the big toe will give many hours of comfort after removal of the toe-nail. Even when general anaesthesia has been used, a nerve block can greatly assist in providing analgesia after surgery.
It should not be expected that the regional anaesthesia will always give excellent analgesia by itself. While it may anaesthetise the wound, pain or discomfort outwith the operative site can still occur e.g. diaphragmatic pain or the presence of a nasogastric tube. However, the reduction in the total amount of pain achieved by the local anaesthetic greatly assists paren-teral analgesic in achieving a high success rate. When using regional anaesthesia postopera-tively, ensure that adequate amounts of analgesics are also prescribed.
Local infiltration
Wound infiltration
Subcutaneous infiltration of the wound by the
surgeon just before skin closure can anaesthetise the skin for many hours. Bupivacaine 0.5% with or without epinephrine 1:200.000 will give several hours of skin anaesthesia. Methods using catheters implanted subcutane-ously, and also in the muscle layers, have been used to allow further injections or a continuous infusion.
Ring block of digits
(Seep. 114and p. 140).
Arthroscopy
(See p. 40). Leaving a small quantity, e.g. 5-10 ml of 0.5% bupivacaine within the knee joint at the completion of arthroscopy will givS good analgesia.
Minor nerve blocks
Iliohypogastric and ilioinguinal nerve blocks
(See p. 44). These blocks are easily performed and can be used for analgesia after hernior-rhaphies.
Foot blocks
(See p. 134). Blockade of the tibial, the superficial and the deep peroneal nerves at the foot will provide analgesia after most foot operations, especially after hallux valgus operations.
Wrist blocks
(See p. 112). These blocks are simple to perform and useful after hand surgery.
Penile block
Penile block after operations such as circumcision is especially useful in children.
Terminal branches of the trigeminal nerves
(See p. 56). These nerves can be blocked after oral or facial surgery.
Major nerve blocks
Brachial plexus block
(See p. 90). This block is very useful after microsurgery of the hand as it not only provides analgesia but also maintains sympathetic blockade and consequent vasodilatation. A catheter such as an IV cannuia can beimplant-ed percutaneously within the neurovascular sheath and repeat injections are then possible.
Femoral nerve block
(See p. 122). This block will give excellent analgesia in patients with a fractured shaft of femur.
Intercostal nerve block
Уважаемый посетитель!
Чтобы распечатать файл, скачайте его (в формате Word).
Ссылка на скачивание - внизу страницы.