Neuromuscular blocking agents
D-tubocurarine and pancuronium, both neuromuscular blocking agents, are administered to improve pulmonary function during artificial ventilation and to reduce pul-
281
monary barotrauma. In newborn rabbits, both drugs cause renal vasoconstriction [67]. The potential adverse effects of these agents on the human newborn kidney should be borne in mind.
Nephrotoxic drugs
Nephrotoxic drugs need special consideration. Because of slow excretion of drugs eliminated by the kidney during the entire neonatal period, toxic blood levels may easily be reached. The nephrotoxicity of aminoglyco-sides, amphotericin B, and radiocontrast agents is mostly due to direct renal cytotoxicity, but additional adverse renal effects can be caused by drug-induced renal vasoconstriction [1]. Aminoglycoside-induced vasoconstriction may be due to increased TXA2 synthesis, whereas aden-osine seems to mediate contrast media-induced renal vasoconstriction [68].
![]() Clinical assessment and
management
Clinical assessment and
management
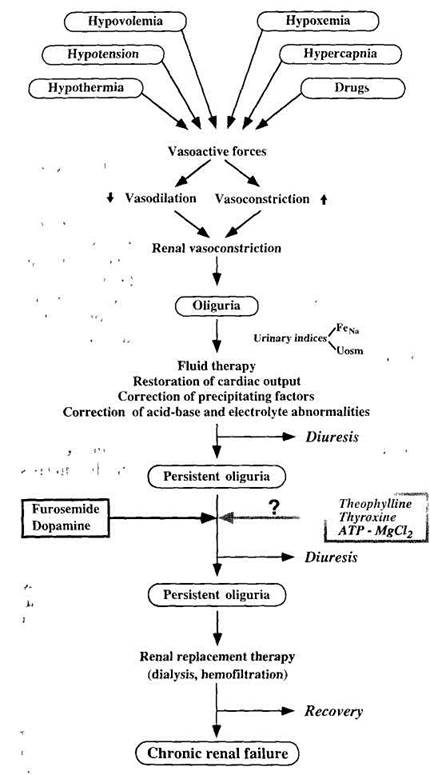
The current diagnostic and therapeutic recommendations regarding neonatal VMNP/ARF place as much emphasis on the prevention of VMNP as on the ultimate treatment of established ARF. The algorithm in Fig. 3 outlines part of the preventive and therapeutic approach. Prevention starts with taking general health measures, aimed at reducing many extrarenal factors that may compromise renal function [69, 70]. The first step is to identify the newborns at risk and place them under careful observation in order to diagnose the occurrence and the cause of oligo-anuria as soon as possible. In case of (incipient) hypovolemia the renal perfusion pressure should be maintained by rapid intravascular volume replacement and (when needed) adequate ventilation, preservation of cardiac output, and avoidance of nephrotoxic drugs [71]. This is, however, easier said than done. It involves trying to improve systemic hemodynamics and renal perfusion by interventions that can also have deleterious effects. Special attention should be given to urine output, which should be measured with a urine collection bag without an indwelling catheter. Bladder catheterization increases the risk of ascending urinary tract infection, with the associated increase in morbidity and mortality. Bladder emptying should be confirmed by cautious supra-pubic pressure, ultrasonographic examination of the bladder, and, if necessary, by intermittent sterile bladder catheterization. Oliguria (<1 ml urine/kg per hour) or anuria is often the first sign of incipient ARF. Renal failure with normal urine output - so-called non-oliguric ARF - is found in about one-third of term newborns with ARF [72] and in 60% of those with ARF in the course of severe asphyxia [36]. Plasma creatinine (PCr) levels should be monitored, otherwise non-oliguric ARF can be missed. In the first days of life PCr is high, reflecting maternal PCr concentrations. The normal high PCr levels may even rise after birth, with a slow decrease during the follow-
232
|
|
Fig. 3 Algorithm of the main pathways for the development and possible interventions/therapy of vasomotor nephropathy in the newborn (FeNa fractional excretion of sodium, Uosm urinary os-molality)
ing 2-3 weeks. The more premature the infant, the higher the PCr. This
Уважаемый посетитель!
Чтобы распечатать файл, скачайте его (в формате Word).
Ссылка на скачивание - внизу страницы.