* THIS PARTICULAR EKG HAS A RATE OF ABOUT 85
|
# Ig squares |
seconds |
rate per minute |
|
i |
0.2 |
300 |
|
2 |
04 |
150 |
|
3 |
06 |
100 |
|
4 |
08 |
75 |
|
5 |
JQ |
60 |
|
6 |
1.2 |
50 |
|
7 |
L4 |
43 |
|
8 |
L6 |
37 |
|
9 |
L8 |
33 |
|
10 |
2fi |
30 |
|
NOTE: Count off the rate as you count off the large squares. As you count the squares from one QRS complex to the next, the rate is 300,150, 100, 75,60 and 50. |
|
|
The other quick method is the scan method. Most manufacturers place markers along the bottom edge of the ECG paper at three second intervals. There are 20 of these three second marker intervals in a minute. Therefore, simply multiply the number of QRS complexes in one three second interval by 20 to obtain the beats per minute. This method is fairly accurate. It may be improved by multiplying the beats in two 3-second intervals by 10. |
|
|
For quick reference, the following are examples of common arrhythmias. Certain stimuli may cause the atrial pacemaker to depolarize at an accelerated rate. When this rate exceeds the normal sinus rate, it pre-empts the normal sinus beat. |
|
|
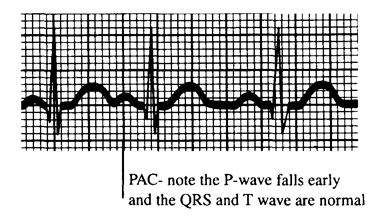
PAC - Premature Atrial Contraction- A single beat that is usually asymptomatic and benign. PACs occur early in the cardiac cycle and may originate from either atrium. The P-wave appears different than the sinus P-wave. The QRS complex and the T wave are usually normal, but if the P-wave appears very early in the cardiac cycle, there may be a prolonged PR interval or even a blocked beat. |
|
|
|
|
|
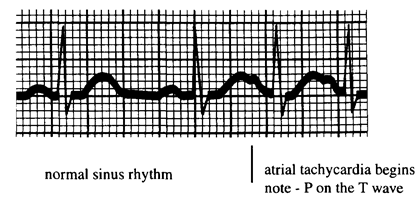
Atrial Tachycardia - May be preceded by frequent PACs, this is a state of continuous discharge from an excited region of the atrium. It usually appears suddenly and subsides just as suddenly. Known as paroxysmal atrial tachycardia (PAT) in the past, it is now known as paroxysmal supra ventricular tachycardia (PSVT). The P waves are abnormal and may be superimposed on the T waves. The rate may range from 120-250 beats per minute. The rhythm is regular with narrow QRS complexes. |
|
|
|
|
|
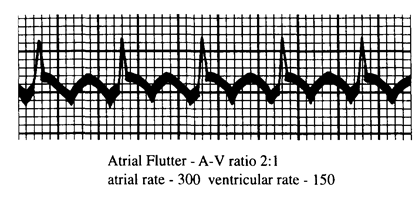
Atrial Flutter - An atrial rate between 250 and 350 beats per minute is characteristic of atrial flutter. When the rate becomes this high the P wave becomes bi-directional and takes on its characteristic saw-toothed appearance. The A-V conduction may remain constant or variable, but the ventricular rate is typically half of the atrial rate or less. |
|
|
|
|
|
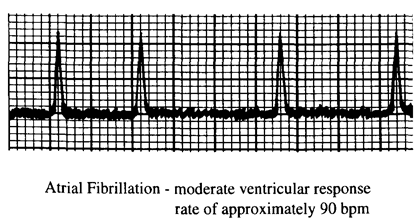
Atrial Fibrillation - The atria can respond to very high rates of impulses. The rate may be so fast with atrial ectopic focus that the atria have not repolarized when the impulse to depolarize arrives. This leads to total disorder of the atria and the loss of their pumping action. The atria quiver as opposed to regular contraction. Ventricular response to these impulses upon the A-V node is random. The ventricular response is irregularly irregular, the hallmark of atrial fibrillation. Atrial fibrillation has three types of ventricular responses. Rapid ventricular response is a ventricular rate over 100. Moderate ventricular response is a ventricular rate of 60 to 100. Slow ventricular response is a ventricular rate of less than 60. The scan method, using the three second markers, is the best way to estimate the ventricular rate due to the irregularity of the rate. |
|
|
|
|
|
There are various rhythm disturbances that may result from conduction of impulses through the A-V conduction system. First degree A-V block is the prolongation of the PR interval greater than 0.20 second (one large block on the ECG paper). This represents a delayed conduction through the atria, A-V node or His-Purkinje fibers. |
|
|
The conduction velocity may become so depressed that some, but not all, impulses fail to penetrate the A-V node. This results in the absence of ventricular depolarization. This is termed second degree A-V block or intermittent A-V block. The relationship of beats that results from atrial stimulus is often referred to as a ratio. For example, if one ventricular contraction occurs for two atrial contractions, second degree A-V block with a 2:1 A-V ratio exists. |
|
|
If no impulses are retransmitted through the A-V node, it is termed third degree or complete A-V block. In this case there may be an impulse from automatic cells farther along the system that stimulates the ventricles. Since the sinus impulse does not reach the ventricles, and the ventricles are receiving impulses from farther along the conduction track, the atria and ventricles may beat at different rates. With complete block and when no impulse is initiated from another source to stimulate the ventricles, cardiac arrest exists. |
|
|
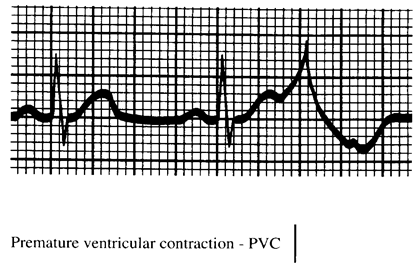
Premature Ventricular Contractions (PVCs) - Premature firing of a ventricular automatic site causes an early beat known as a PVC. This beat is defined as having no P wave, a wide QRS complex (>0.12sec), and it must be followed by a compensatory pause. Bigeminy is where every sinus beat is followed by a PVC. Two sinus beats followed by a PVC are refered to as trigeminy. Two consecutive PVCs are couplets. Three or more consecutive PVCs are considered ventricular tachycardia. |
|
|
|
|
|
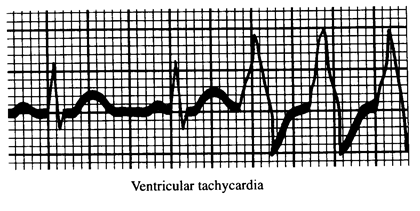
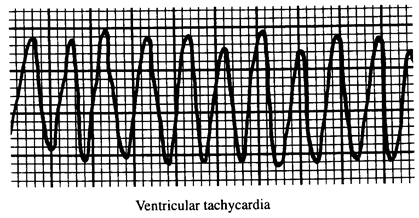
Ventricular Tachycardia (VT) - A series of impulses from automatic cells within the ventricles, at a rate that is more rapid than the normal ventricular rate (20 - 50 bpm). VT may be sustained (persists more than 30 seconds) or nonsustained. Ventricular tachycardia consists of A-V dissociation, QRS complexes that are abnormally wide and of different form, and a rate exceeding 100 beats per minute. Extremely high ventricular rates cause the merging of the QRS and T waves producing a sine wave. The ventricular contraction time is short, and there is inadequate time for the chambers to fill. Cardiac output becomes inadequate and circulatory failure ensues. Without immediate intervention, this usually leads to ventricular fibrillation and cardiac death. |
|
|
|
|
|
|
|
|
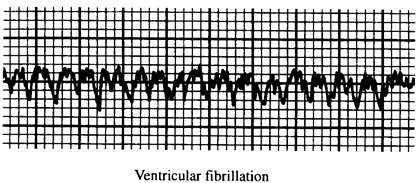
Ventricular Fibrillation (VF) - When the ventricular impulses become so rapid they cannot be processed, the condition is known as ventricular fibrillation. The onset usually begins with a short run of VT. Like atrial fibrillation, the muscles of the ventricles are depolarizing at different times throughout. The ventricles quiver throughout instead of contracting. Without immediate treatment this is fatal. |
|
|
|
|
|
Nervous System Control |
Нервная система |
|
The autonomic nervous system is the major factor outside of the heart itself that influences the actions of the heart. The SA node discharge is under the influence of the sympathetic and parasympathetic (vagal) |
|
|
divisions of the nervous system. Although the node will discharge spontaneously if no nervous system influence is present, it is affected by these systems. The main regulation of the heart rate is done by the balancing of the sympathetic discharges, which increase the rate, and of the parasympathetic discharges, which slow the rate. |
|
|
The catecholamine level will increase as the sympathetic system is activated. The catecholamine that influences this system is norepinephrine. This increase of the circulating catecholamines will increase both the heart rate and force of contractions. An inotropic response to sympathetic stimulation will be exhibited by the left ventricle. |
|
|
Contractility of the myocardium is controlled by reflex responses from chemoreceptors and mechanoreceptors. Sympathetic and parasympathetic nerves transmit information to cause changes in the heart rate and contractility. Chemoreceptors are found in the carotid and aortic bodies. These receptors are stimulated by decreasing pO, increasing pCO^, or decreasing pH. The heart rate, arterial pressure and left ventricular inotropy are all influenced by arterial baroreceptors. Left ventricular inotropy, however, is much less influenced than the heart rate and arterial pressure. |
|
|
Exercise causes sympathetic stimulation and decreased parasympathetic activity. Hemorrhage causes sympathetic activity to increase the arterial pressure and heart rate. Left ventricular inotropy is, again, much less influenced. |
|
|
Parasympathetic stimulation decreases heart rate, cardiac output and peripheral resistance. This inhibitory part of the nervous system works to decrease the effects of the sympathetic system. Acetylcholine is the chemical that is involved in stimulation of the parasympathetic system. The interaction of the sympathetic and parasympathetic systems is a complex one. Parasympathetic influence on the sympathetic effects can occur at different levels. This influence can work between nerve endings at the prejunctional level to decrease the amount of norepinephrine released from sympathetic nerve terminals. The parasympathetic influence can also work at the postjunctional level. Muscarinic receptors are activated to decrease the effect of cardiac myocytes to beta-adrenergic stimulation. The parasympathetic effect is magnified in the presence of sympathetic activity. |
Уважаемый посетитель!
Чтобы распечатать файл, скачайте его (в формате Word).
Ссылка на скачивание - внизу страницы.